Last updated on January 4th, 2025 at 09:54 pm
Myasthenia gravis (MG) is a complex autoimmune disorder affecting the neuromuscular junction, characterized by fluctuating muscle weakness that worsens with activity and improves with rest. As a nurse, understanding the intricacies of this condition is crucial for providing optimal patient care. This comprehensive guide will explore the nursing diagnoses, care plans, and interventions essential for managing patients with myasthenia gravis.
Understanding Myasthenia Gravis
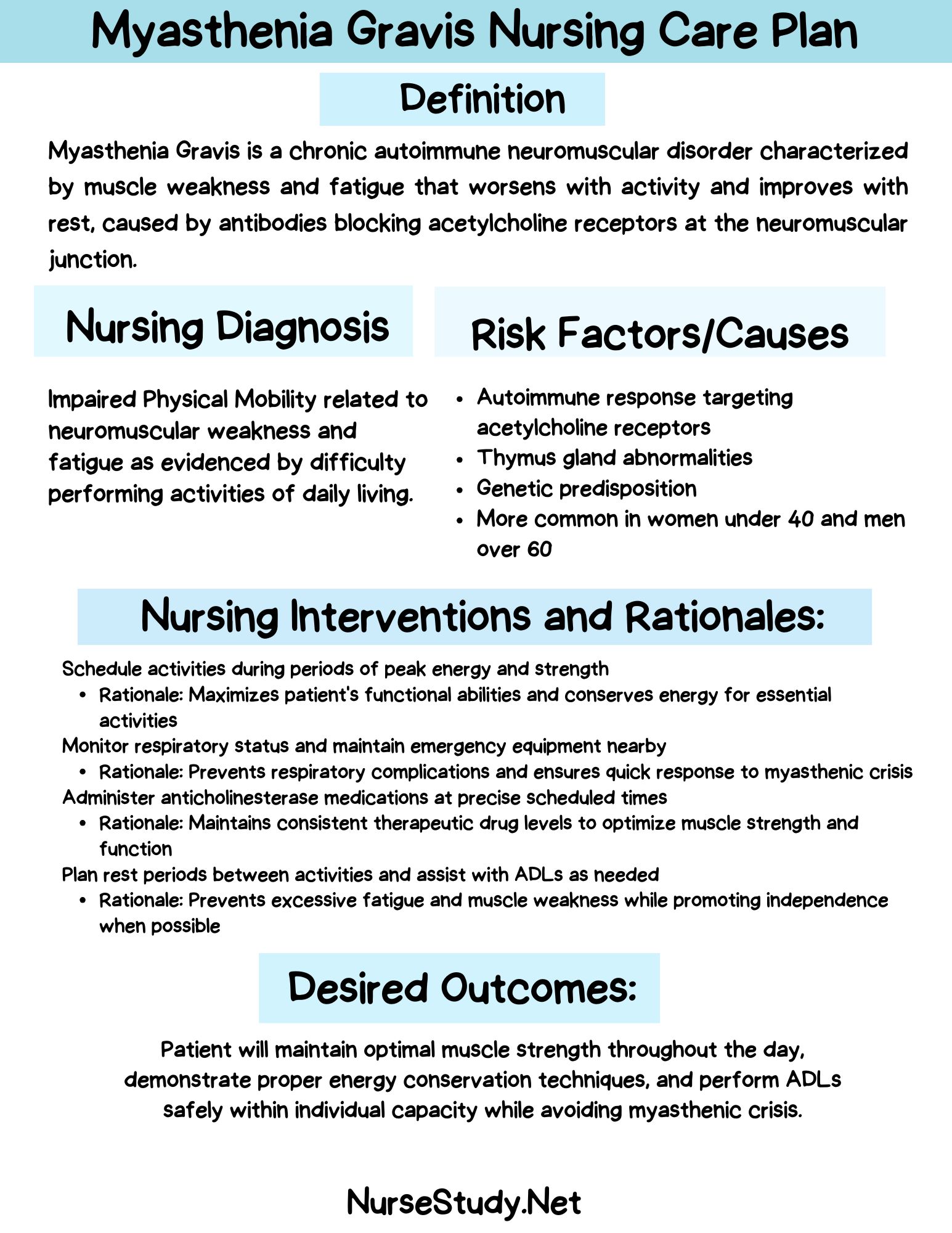
Myasthenia gravis occurs when antibodies attack the neuromuscular junction’s acetylcholine receptors (AChR). This attack results in fewer functional AChRs, inhibiting acetylcholine’s ability to effectively stimulate muscle contractions. The hallmark symptom of MG is fluctuating skeletal muscle weakness, which can affect various muscle groups, including those controlling eye movements, facial expressions, chewing, breathing, and speaking.
The course of MG is highly variable. Some patients may experience periods of remission, while others may develop severe symptoms or face life-threatening complications. Factors that can exacerbate MG symptoms include pregnancy, trauma, illness, stress, extreme temperature changes, and electrolyte imbalances like hypokalemia.
Diagnosis of MG typically involves a combination of clinical history, physical examination, and diagnostic tests such as electromyography (EMG) or the edrophonium (Tensilon) test.
The Nursing Process in Myasthenia Gravis Care
As MG is a chronic and progressive condition, the role of nurses is crucial in supporting patients through ongoing assessments, implementing treatment interventions, and providing comprehensive patient education. The nursing process for MG patients focuses on:
- Conducting thorough assessments to monitor disease progression and identify potential complications
- Implementing interventions to manage symptoms and prevent exacerbations
- Educating patients and caregivers about the disease, its management, and potential complications
- Providing emotional support and resources to cope with the chronic nature of the condition
Nursing Care Plans for Myasthenia Gravis
Nursing care plans are essential for prioritizing assessments and interventions to achieve both short-term and long-term care goals for patients with myasthenia gravis. Here are five key nursing care plans for managing MG:
Nursing Care Plan 1. Impaired Physical Mobility
Nursing Diagnosis Statement: Impaired Physical Mobility related to muscle weakness and fatigue secondary to myasthenia gravis as evidenced by difficulty performing activities of daily living, decreased range of motion, and verbalized fatigue.
Related factors/causes:
- Neuromuscular impairment
- Decreased muscle strength
- Fatigue
Nursing Interventions and Rationales:
- Assess the patient’s level of mobility and strength at regular intervals throughout the day.
Rationale: This helps identify patterns of weakness and guide activity planning. - Assist the patient in developing an energy conservation plan.
Rationale: Helps the patient manage activities to prevent excessive fatigue. - Collaborate with physical and occupational therapists to develop an appropriate exercise and mobility program.
Rationale: Tailored exercise programs can help maintain muscle strength without causing excessive fatigue. - Educate the patient on the importance of rest periods between activities.
Rationale: Rest allows for muscle recovery and helps prevent exacerbation of symptoms. - Provide assistive devices as needed (e.g., walker, wheelchair) and teach proper use.
Rationale: Assistive devices can help conserve energy and promote safe mobility.
Desired Outcomes:
- The patient will demonstrate improved mobility within their limitations
- The patient will verbalize understanding of energy conservation techniques
- Patient will safely use assistive devices when necessary
Nursing Care Plan 2. Ineffective Breathing Pattern
Nursing Diagnosis Statement: Ineffective Breathing Pattern related to respiratory muscle weakness secondary to myasthenia gravis as evidenced by shortness of breath, use of accessory muscles, and decreased vital capacity.
Related factors/causes:
- Neuromuscular impairment of respiratory muscles
- Fatigue
- Ineffective cough reflex
Nursing Interventions and Rationales:
- Assess respiratory rate, depth, and pattern regularly.
Rationale: Early detection of respiratory changes can prevent complications. - Position the patient in a semi-Fowler’s or high Fowler’s position.
Rationale: This position promotes optimal lung expansion and eases breathing effort. - Teach and encourage deep breathing and coughing exercises.
Rationale: These exercises help maintain airway clearance and prevent atelectasis. - Monitor oxygen saturation levels and administer oxygen as prescribed.
Rationale: Ensures adequate oxygenation and early detection of respiratory compromise. - Prepare for and assist with non-invasive ventilation if prescribed.
Rationale: Non-invasive ventilation can support respiratory function during periods of weakness.
Desired Outcomes:
- The patient will maintain oxygen saturation within normal limits
- The patient will demonstrate improved respiratory pattern and depth
- The patient will effectively perform deep breathing and coughing exercises
Nursing Care Plan 3. Risk for Aspiration
Nursing Diagnosis Statement: Risk for Aspiration related to impaired swallowing mechanism secondary to myasthenia gravis.
Related factors/causes:
- Weakness of oropharyngeal muscles
- Impaired gag reflex
- Fatigue during meals
Nursing Interventions and Rationales:
- Assess swallowing ability before meals and medication administration.
Rationale: Swallowing ability can fluctuate throughout the day in MG patients. - Position the patient in an upright sitting position during and for 30 minutes after meals.
Rationale: This position reduces the risk of aspiration. - Provide small, frequent meals and thickened liquids as a speech therapist recommends.
Rationale: Smaller meals and thickened liquids are easier to manage and reduce aspiration risk. - Teach the patient to take small bites, chew thoroughly, and swallow carefully.
Rationale: These techniques help compensate for muscle weakness and reduce aspiration risk. - Have suction equipment readily available.
Rationale: Allows for prompt clearance of secretions if needed.
Desired Outcomes:
- The patient will demonstrate safe swallowing techniques.
- The patient will maintain adequate nutrition without aspiration events
- The patient will verbalize understanding of aspiration prevention strategies
Nursing Care Plan 4. Self-Care Deficit
Nursing Diagnosis Statement: Self-Care Deficit related to muscle weakness and fatigue secondary to myasthenia gravis as evidenced by inability to complete activities of daily living independently.
Related factors/causes:
- Neuromuscular impairment
- Fatigue
- Weakness in extremities
Nursing Interventions and Rationales:
- Assess the patient’s ability to perform self-care activities at different times of the day.
Rationale: MG symptoms can fluctuate, affecting self-care abilities. - Assist with self-care activities as needed, encouraging independence when possible.
Rationale: Promotes independence while ensuring safety and completion of necessary tasks. - Provide adaptive equipment (long-handled sponges, electric toothbrushes) and teach them how to use them.
Rationale: Adaptive equipment can help conserve energy and promote independence. - Schedule self-care activities during periods of peak strength.
Rationale: Aligning activities with periods of greater strength improves success and reduces fatigue. - Collaborate with occupational therapy for personalized self-care strategies.
Rationale: Occupational therapists can provide specialized techniques and equipment recommendations.
Desired Outcomes:
- The patient will demonstrate increased independence in self-care activities
- The patient will use adaptive equipment effectively
- The patient will verbalize satisfaction with self-care management
Nursing Care Plan 5. Knowledge Deficit
Nursing Diagnosis Statement: Knowledge Deficit related to lack of information about myasthenia gravis management as evidenced by verbalized misconceptions and questions about the disease process and treatment.
Related factors/causes:
- Lack of exposure to information about MG
- The complexity of the disease and its management
- Misunderstanding of medication regimens
Nursing Interventions and Rationales:
- Assess the patient’s current understanding of myasthenia gravis and its management.
Rationale: Identifies knowledge gaps and guides education planning. - Provide comprehensive education about MG, including symptoms, triggers, and management strategies.
Rationale: This helps the patient to actively participate in their care and recognize potential exacerbations. - Teach the importance of medication adherence and potential side effects.
Rationale: Proper medication management is crucial for symptom control in MG. - Instruct on the signs and symptoms of myasthenic crisis and when to seek immediate medical attention.
Rationale: Early recognition of a crisis can be life-saving. - Provide written materials and reliable online resources for ongoing reference.
Rationale: Reinforces verbal education and provides a resource for future questions.
Desired Outcomes:
- The patient will verbalize understanding of myasthenia gravis and its management.
- The patient will demonstrate proper medication administration techniques
- The patient will identify signs of exacerbation and appropriate actions to take
Conclusion
Effective nursing care for patients with myasthenia gravis requires a comprehensive understanding of the disease process, potential complications, and individualized patient needs. By implementing these nursing care plans and remaining vigilant for patient condition changes, nurses can significantly improve outcomes and quality of life for individuals living with MG.
References
- Gilhus, N. E., & Verschuuren, J. J. (2015). Myasthenia gravis: subgroup classification and therapeutic strategies. The Lancet Neurology, 14(10), 1023-1036.
- Hehir, M. K., & Silvestri, N. J. (2018). Generalized Myasthenia Gravis: Classification, Clinical Presentation, Natural History, and Epidemiology. Neurologic Clinics, 36(2), 253-260.
- Melzer, N., Ruck, T., Fuhr, P., Gold, R., Hohlfeld, R., Marx, A., … & Wiendl, H. (2016). Clinical features, pathogenesis, and treatment of myasthenia gravis: a supplement to the Guidelines of the German Neurological Society. Journal of Neurology, 263(8), 1473-1494.
- Norwood, F., Dhanjal, M., Hill, M., James, N., Jungbluth, H., Kyle, P., … & Hilton-Jones, D. (2014). Myasthenia in pregnancy: best practice guidelines from a UK multispecialty working group. Journal of Neurology, Neurosurgery & Psychiatry, 85(5), 538-543.
- Sanders, D. B., Wolfe, G. I., Benatar, M., Evoli, A., Gilhus, N. E., Illa, I., … & Kaminski, H. J. (2016). International consensus guidance for management of myasthenia gravis: Executive summary. Neurology, 87(4), 419-425.
- Wendell, L. C., & Levine, J. M. (2011). Myasthenic crisis. The Neurohospitalist, 1(1), 16-22.